Laparoscopic Anti-reflux Surgery
 General
General
Gastro-esophageal reflux disease (GERD) is a very common condition which has become more frequent the last few decades due to its association with obesity. In addition, GERD is also associated with diaphragmatic hernias (link to “laparoscopic diaphragmatic hernia repair”). Diaphragmatic hernias represent a special category of abdominal hernias which are located at the natural diaphragmatic hiatus which naturally exists and permits the entrance of esophagus and great vessels from the thoracic to the abdominal cavity. When the hiatus enlarges it may allow the herniation of part of the stomach or other abdominal organs to the thoracic cavity.
Symptoms and diagnosis
GERD usually presents with heartburn, regurgitation, painful swallowing, hoarseness and with a clinical picture of asthma or pneumonia. Diagnosis is usually made by barium swallow, gastroscopy and 24-hour pH study.
Procedure and postoperative course
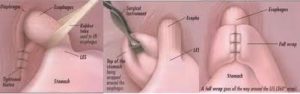
According to Professor Raftopoulos’ experience laparoscopic diaphragmatic hernia repair is performed through five small incision 2-4 cm or 1 to 1 and ¾ inches long. If a diaphragmatic hernia co-exists this is repaired and GERD is addressed with a type of fundoplication, most commonly Nissen fundoplication. If the patient is also morbidly obese, then laparoscopic Roux-en-Y gastric bypass (link to “laparoscopic Roux-en-Y gastric bypass”) may be considered as an alternative treatment. Hospital stay is usually 1-2 days. Postoperative pain is usually controlled with Paracetamol or Acetaminophen. Return to work is usually possible within 7 days from surgery.
Complications
Laparoscopic antireflux surgery is not usually associated with complications. Occasionally a pneumothorax may occur if the pleural space is accidentally violated during surgery. Postoperatively routine radiologic surveillance of the repair is recommended to detect hernia recurrence if a diaphragmatic hernia was repaired. If fundoplications are too “tight” then dysphagia may occur and require endoscopic balloon dilation. In addition, due to the fundoplication a “gas-bloating” syndrome may occur. Such side-effects usually improve over time.
Professor Raftopoulos’ experience
Dr. Raftopoulos has extensive experience in antireflux surgery. This experience originates by the fact that diaphragmatic hernias are very frequent in obese patients and require concomitant repair during bariatric surgery. Although these repairs are technically challenging, they can be performed safely if such experience exists. In addition, Professor Raftopoulos has published his experience with laparoscopic antireflux surgery in peer reviewed medical journals such as the treatment of GERD in morbidly obese patients with laparoscopic gastric bypass at the Obesity Surgery journal, and laparoscopic antireflux surgery and diaphragmatic hernia repair at the Surgical Endoscopy journal. For more information please contact our office.